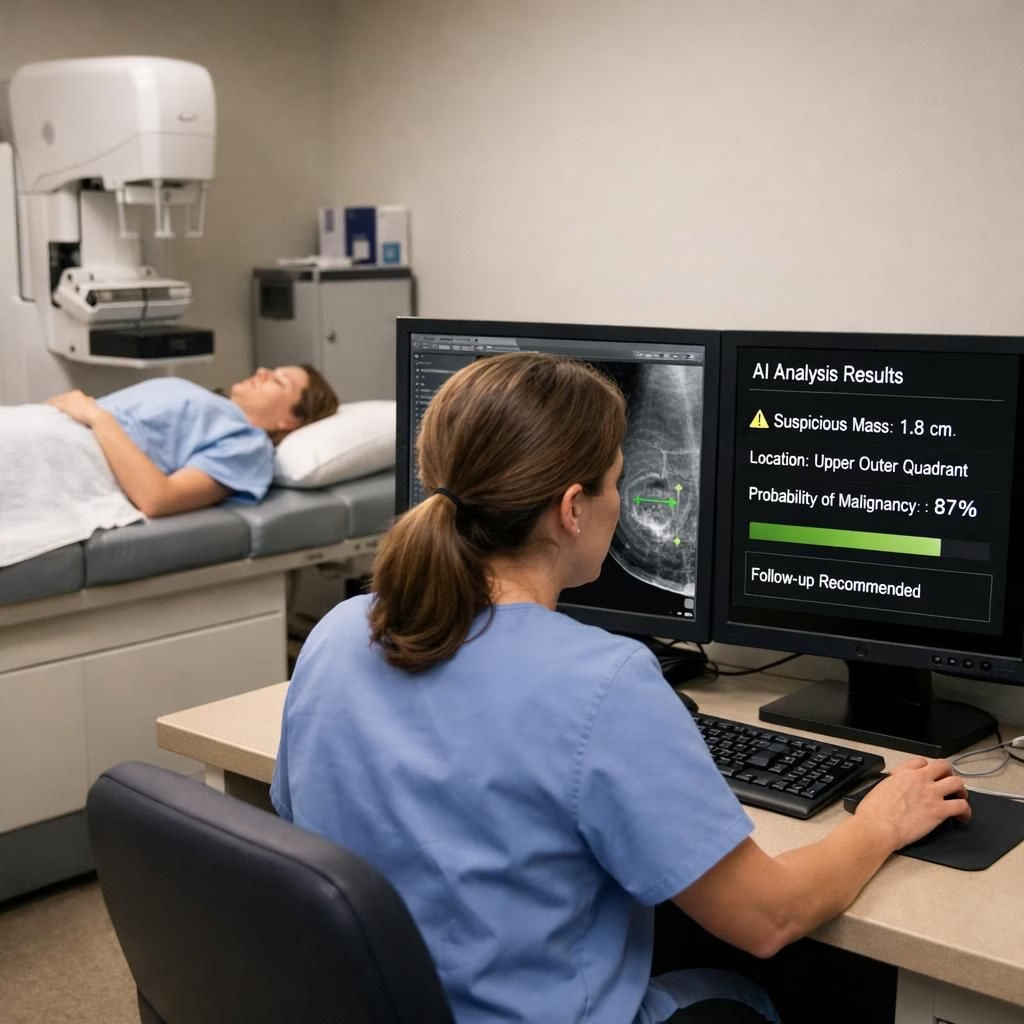
During a Crain’s New York Business panel, the CEO of NYC Health + Hospitals floated a bold idea: AI could read imaging studies in the near term and, over time, reshape radiology workflows. He caveated that regulatory rules must catch up and that patient safety always comes first, but the core impulse was clear: expand access, trim delays, and drive costs out of imaging processes where it makes sense. He pointed specifically to breast cancer screening, arguing that automated reads could speed up triage and reduce unnecessary follow-ups, thereby enabling earlier intervention for more patients. The moment captured a broad trend: the tech industry’s optimism about automation as a way to solve real health care bottlenecks, clashing with frontline clinicians’ worries about accuracy, accountability, and the delicate art of human judgment in interpretation.
The debate is not just about gadgets; it is about trust, safety, and who bears responsibility when something goes wrong. Advocates point to the potential to expand access to screenings and to standardize results across sites. Critics push back with concerns about accuracy, edge cases, and the patient experience. Regulators will need to define safety nets, validation standards, and clear pathways for adoption, ideally with real-world pilots and careful monitoring. In radiology policy settings, regulators must define those safety nets and reporting standards to build clinician and patient confidence.
AI in radiology: promises, pitfalls, and policy
In practical terms, the fairest path would blend automated triage with strong human oversight in radiology workflows. The aim would be to cut wait times and increase screening throughput while keeping patient safety front and center. In early stages, automated flags could highlight potential abnormalities on mammograms or X-rays, with clinicians confirming outcomes. The human-in-the-loop approach tends to produce steady gains without surrendering essential professional judgment.
Radiology and AI: practical adoption and safety risks
From a policy standpoint, the road ahead requires shared guidelines, transparent validation, and patient-centered risk communication. Present-day capabilities offer modest efficiencies at best; sweeping claims about transformation are often overstated. Yet there is value in pursuing steady improvements, as long as oversight, data quality, and accountability stay in focus in radiology.
The broader conversation between tech and medicine is ongoing and evolving. Leading executives have sparked discussions about where automation might fit into care delivery, while clinicians emphasize that practice realities outpace hype. A clinician working in imaging has cautioned against overstatement, noting that the core workflow remains challenging beyond basic triage and detection tasks. The takeaway: innovation should be guided by evidence, not by novelty alone. In radiology practice, that cautious approach is especially warranted.
Looking ahead to 2026, hospitals will need pilots, sandboxed trials, and meaningful collaboration among regulators, clinicians, and developers. Real-world validation, interoperability, and clear reporting will guide decisions more than headlines. If automation can genuinely improve access to screening without compromising accuracy, it deserves a place as a powerful tool rather than a wholesale replacement for expertise in radiology.
What do you think? Share your thoughts in the comments.
Source attribution: Thank you to Crain’s New York Business for the original reporting. Original article: Crain’s New York Business.
External sources
- FDA: AI and ML in medical devices
- ACR Facts: AI in Radiology
- Nature: AI in radiology and human oversight
References
Times of India article (original source): Times of India — technology news summary